15 Sep

Blood Pressure During Steroids
Table of contents:
2.1 - Retention of water and sodium
2.2 - Lees no, rigid arterials
2.3 - Pressure and sympathetic system
2.4 - Pressure and grow of the heart
2.5 - Cholesterol
2.6 - What the science says?
2.2 - Lees no, rigid arterials
2.3 - Pressure and sympathetic system
2.4 - Pressure and grow of the heart
2.5 - Cholesterol
2.6 - What the science says?
3.1 - Oxymetholone
3.2 - Dianabol
3.3 - Trenbolone
3.4 - Nandrolone
3.5 - Boldenone
3.6 - Testosterone
3.2 - Dianabol
3.3 - Trenbolone
3.4 - Nandrolone
3.5 - Boldenone
3.6 - Testosterone
1 - What is blood pressure
Blood pressure is the numerical expression of the force exerted by blood against the walls of the arteries while the heart works tirelessly to deliver oxygen and nutrients to every cell of your body.
When you read a figure like 120/80 mmHg, what you have in front of you is a summary of how your cardiovascular system is functioning:
-The first number, the systolic, reflects the maximum pressure during contraction of the left ventricle, that pumps blood into the aorta.
-The second number, the diastolic, tells us about the pressure when the heart relaxes and fills again: it reveals much about the condition of your arteries and their resistance to flow.
It is a number that sums up the work of your heart, the tone of your arteries, the blood viscosity, the volume of fluid in your system. In short, it is a vital marker. In the world of steroid use, this figure can go from being a routine value to a danger sign if not properly monitored and controlled.
When you read a figure like 120/80 mmHg, what you have in front of you is a summary of how your cardiovascular system is functioning:
-The first number, the systolic, reflects the maximum pressure during contraction of the left ventricle, that pumps blood into the aorta.
-The second number, the diastolic, tells us about the pressure when the heart relaxes and fills again: it reveals much about the condition of your arteries and their resistance to flow.
It is a number that sums up the work of your heart, the tone of your arteries, the blood viscosity, the volume of fluid in your system. In short, it is a vital marker. In the world of steroid use, this figure can go from being a routine value to a danger sign if not properly monitored and controlled.

2 - How affect the steroids
The increase in blood pressure among steroid users is no coincidence, nor is it an isolated effect: it is the result of a series of physiological mechanisms that AAS (Anabolic-Androgenic Steroids) trigger, both directly and indirectly. Let’s break it down so you can understand each link in this chain:
2.1 - Retention of water and sodium
Many steroids, especially those derived from nandrolone (such as trenbolone) or methylated orals (such as Dianabol or oxymetholone), generate an effect similar to mineralocorticoid hormones (like aldosterone).
This causes your kidneys to reabsorb more sodium than usual, and with it, water.
The result? The volume of blood circulating through your system increases, the pressure against the vessel walls rises, and the heart must pump harder.
Plasma volume expansion particularly elevates systolic pressure. While this may seem like a transient effect at first, over time it causes continuous stress on the arteries and the heart muscle itself.
2.2 - Lees no, rigid arterials
The endothelium is like the “intelligent” inner layer of your blood vessels. It doesn’t just line them, it actively regulates vascular tone through the production of nitric oxide (NO), a key molecule to keep arteries relaxed and blood flow smoothly.
Steroids impair this capacity of the endothelium to produce NO. At the same time, they increase the synthesis of endothelin-1, a potent vasoconstrictor. This means your arteries lose elasticity, become “stiffer,” and their diameter narrows. Increasing resistance to blood flow (i.e peripheral vascular resistance), steadily increasing diastolic pressure. Endothelial dysfunction is the first step toward a dangerous path: that of atherosclerosis and chronic organ damage.
Steroids impair this capacity of the endothelium to produce NO. At the same time, they increase the synthesis of endothelin-1, a potent vasoconstrictor. This means your arteries lose elasticity, become “stiffer,” and their diameter narrows. Increasing resistance to blood flow (i.e peripheral vascular resistance), steadily increasing diastolic pressure. Endothelial dysfunction is the first step toward a dangerous path: that of atherosclerosis and chronic organ damage.
2.3 - Pressure and sympathetic system
Steroids alter the balance of the autonomic nervous system, pushing it toward the sympathetic side — the one that activates in fight or flight situations. This results in the chronic release of catecholamines like adrenaline and noradrenaline.
The effect? More contracted vessels, a heart that beats faster and stronger, a system in constant tension. This state not only chronically raises BP but also favors the appearance of arrhythmias, especially if combined with the pathological growth of the left ventricle that we will now see.
The effect? More contracted vessels, a heart that beats faster and stronger, a system in constant tension. This state not only chronically raises BP but also favors the appearance of arrhythmias, especially if combined with the pathological growth of the left ventricle that we will now see.
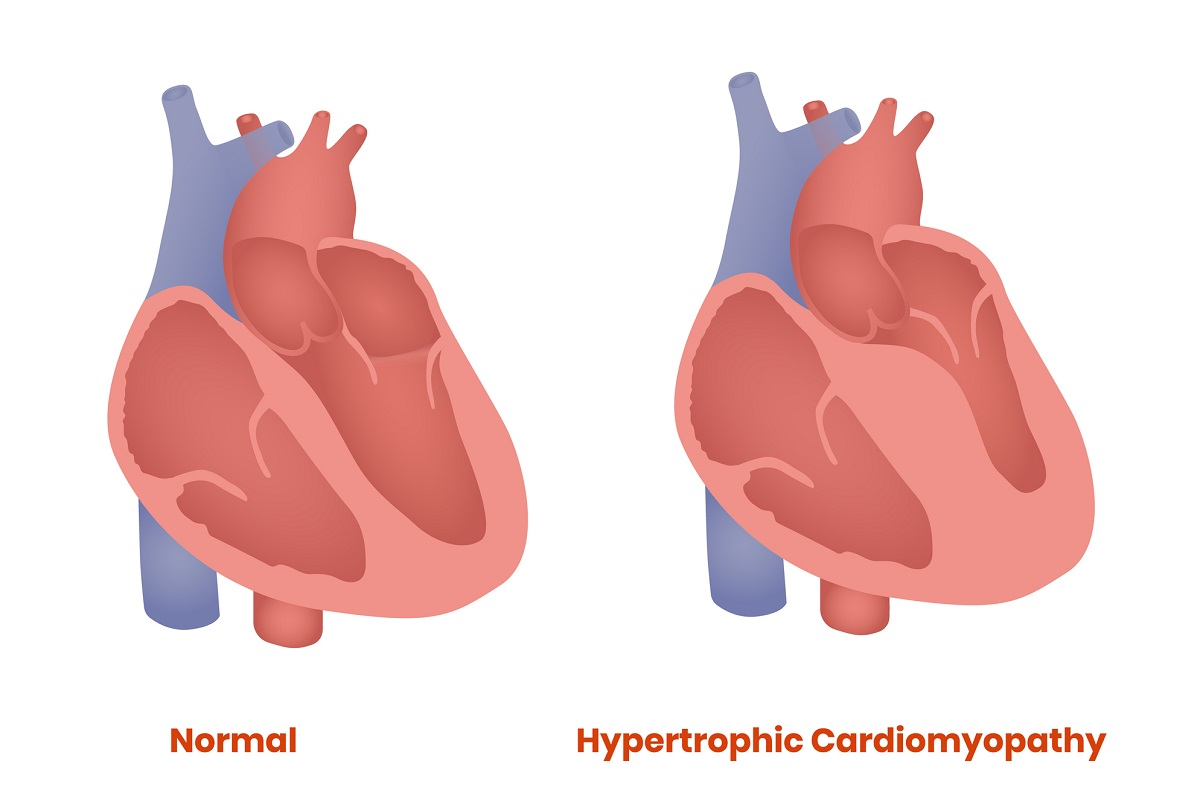
2.4 - Pressure and grow of the heart
Your heart is a muscle, and like any muscle, it grows in response to overexertion. But in the case of the left ventricle, this growth isn’t necessarily beneficial.
Left ventricular hypertrophy induced by the combination of hypertension and the direct anabolic effect of AAS means the ventricle wall thickens at the expense of reducing cavity size and relaxation capacity. 👉 This results in a stiffer, less efficient heart that over time can lead to heart failure with preserved ejection fraction and an increased risk of potentially fatal arrhythmias.
Left ventricular hypertrophy induced by the combination of hypertension and the direct anabolic effect of AAS means the ventricle wall thickens at the expense of reducing cavity size and relaxation capacity. 👉 This results in a stiffer, less efficient heart that over time can lead to heart failure with preserved ejection fraction and an increased risk of potentially fatal arrhythmias.
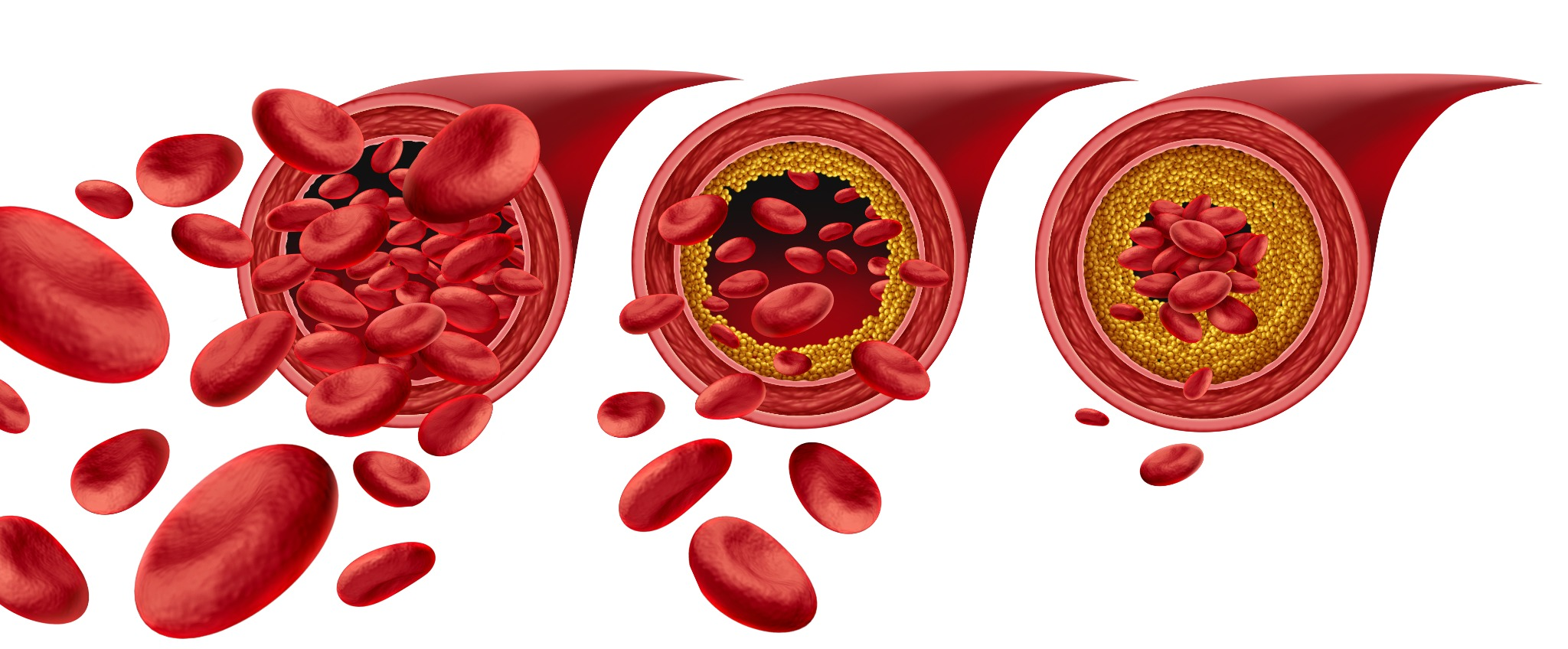
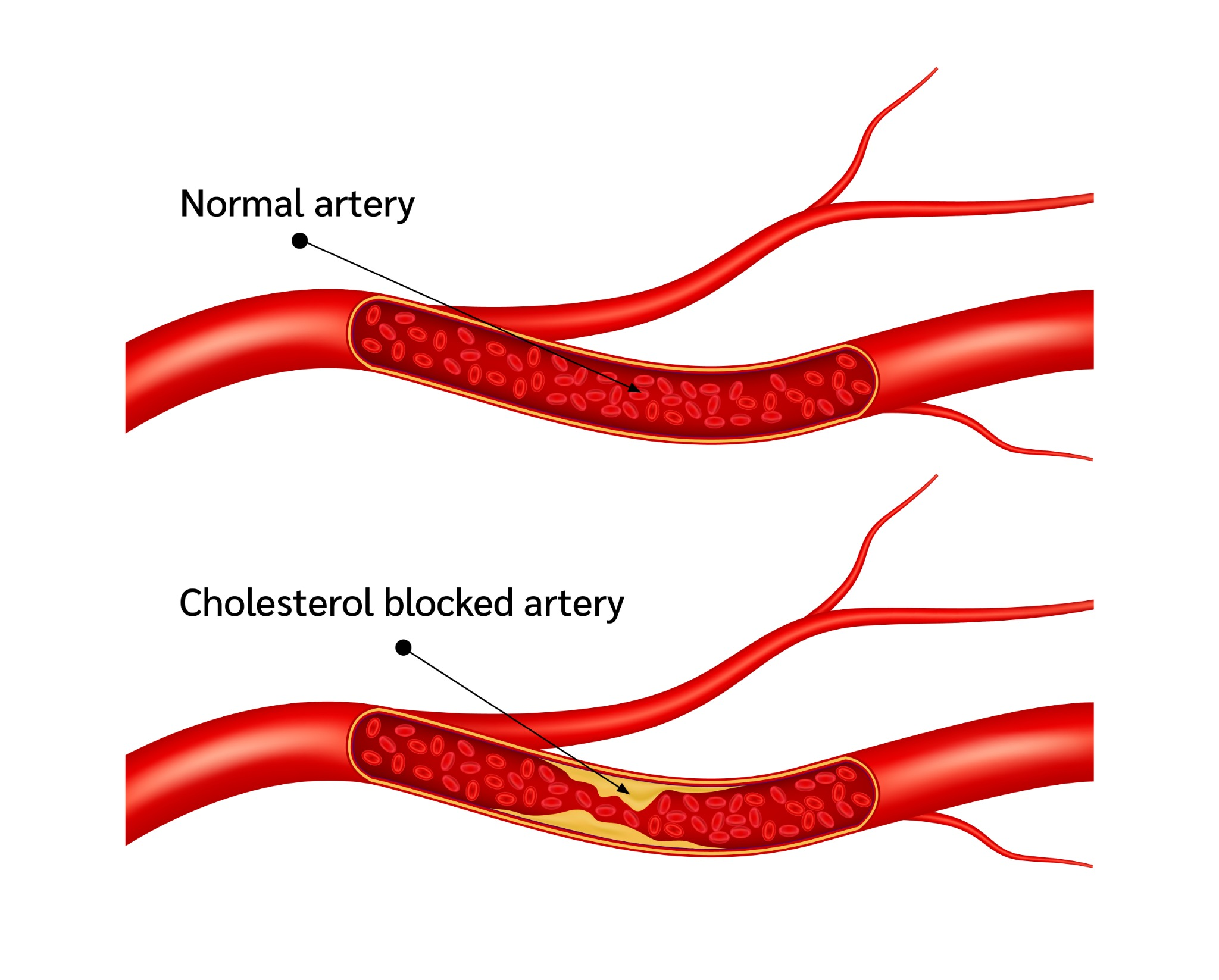
2.5 - Cholesterol
AAS, especially at supraphysiological doses, crash HDL-C levels (the so-called “good” cholesterol) and raise LDL-C and oxidized LDL levels.
This worsens the lipid profile, encouraging the formation of atheroma plaques, those accumulations of fat and inflammatory cells that narrow your arteries and make them stiffer and more fragile. As a result, blood pressure stays high not only due to volume or vascular tone, but because the arteries themselves lose their ability to adapt to blood flow changes.
This worsens the lipid profile, encouraging the formation of atheroma plaques, those accumulations of fat and inflammatory cells that narrow your arteries and make them stiffer and more fragile. As a result, blood pressure stays high not only due to volume or vascular tone, but because the arteries themselves lose their ability to adapt to blood flow changes.
2.6 - What the science says?
Scientific literature is clear. Studies on steroid users show average increases of 10-20 mmHg in systolic and 5-15 mmHg in diastolic, depending on the type, dose, and duration of the cycle.
But the most alarming part? These increases do not always disappear after stopping the cycle, especially if cycles have been prolonged or involved substances particularly aggressive for the cardiovascular system.
The combination of steroids with other substances (GH, clenbuterol, T3) further enhances the hypertensive effect and cardiovascular damage.
One of the most common mistakes in bodybuilding and sports pharmacology is assuming all steroids affect blood pressure the same. Nothing could be further from the truth. The hypertensive impact of an AAS depends on many factors: its chemical structure (which family it belongs to: testosterone, DHT, 19-nor...), its affinity for mineralocorticoid receptors, its effect on sodium-potassium balance, its ability to alter lipid profile, and of course, its dose and administration route.
One of the most common mistakes in bodybuilding and sports pharmacology is assuming all steroids affect blood pressure the same. Nothing could be further from the truth. The hypertensive impact of an AAS depends on many factors: its chemical structure (which family it belongs to: testosterone, DHT, 19-nor...), its affinity for mineralocorticoid receptors, its effect on sodium-potassium balance, its ability to alter lipid profile, and of course, its dose and administration route.
3 - Worst steroids for blood pressure
3.1 - Oxymetholone
If there is a compound that deserves the number one spot in the hypertensive steroid ranking, it’s oxymetholone.
This oral, originally designed to treat severe anemias, is extremely effective for weight gain… but much of that weight is retained water. 👉 Why does it raise BP so much?
-It has a strong indirect mineralocorticoid effect, promoting significant sodium and water retention at the renal level. This rapidly and uncontrollably expands plasma volume.
-Increases cardiac output because the heart has to pump a greater volume of blood.
-Dramatically alters the lipid profile, crashing HDL and raising LDL, accelerating endothelial damage and artery stiffening.
-Induces endothelial dysfunction, reducing NO production and promoting vasoconstriction.
As a result, users report systolic BP increases of 10-30 mmHg in a few weeks. The puffy face, prominent veins despite retention, and feeling of cranial pressure are classic signs.
This oral, originally designed to treat severe anemias, is extremely effective for weight gain… but much of that weight is retained water. 👉 Why does it raise BP so much?
-It has a strong indirect mineralocorticoid effect, promoting significant sodium and water retention at the renal level. This rapidly and uncontrollably expands plasma volume.
-Increases cardiac output because the heart has to pump a greater volume of blood.
-Dramatically alters the lipid profile, crashing HDL and raising LDL, accelerating endothelial damage and artery stiffening.
-Induces endothelial dysfunction, reducing NO production and promoting vasoconstriction.
As a result, users report systolic BP increases of 10-30 mmHg in a few weeks. The puffy face, prominent veins despite retention, and feeling of cranial pressure are classic signs.

3.2 - Dianabol
The legendary Dianabol, the old-school favorite, is also one of the most problematic steroids for blood pressure.
Mechanisms:
High water retention due to its indirect mineralocorticoid action. Sodium accumulates, water follows, and intravascular volume skyrockets.
Severe alteration of the lipid profile: crashed HDL, elevated LDL, promoting atheroma plaques and reducing arterial elasticity.
Marked endothelial dysfunction: reduction of NO and increase of endothelin-1.
In heavy Dianabol cycles, it’s not uncommon to see blood pressure levels in the 140-160 mmHg systolic range if sodium isn’t controlled and cardio is neglected.
Mechanisms:
High water retention due to its indirect mineralocorticoid action. Sodium accumulates, water follows, and intravascular volume skyrockets.
Severe alteration of the lipid profile: crashed HDL, elevated LDL, promoting atheroma plaques and reducing arterial elasticity.
Marked endothelial dysfunction: reduction of NO and increase of endothelin-1.
In heavy Dianabol cycles, it’s not uncommon to see blood pressure levels in the 140-160 mmHg systolic range if sodium isn’t controlled and cardio is neglected.

3.3 - Trenbolone
Trenbolone is the steroid many consider the “king” of hypertrophy, but also the king of cardiovascular damage.
What makes it so aggressive for BP?
-Intense indirect mineralocorticoid effect: although it doesn’t bind to classic mineralocorticoid receptors like aldosterone, it alters sodium-potassium balance and promotes sodium retention.
-Chronic vasoconstriction: trenbolone enhances sympathetic nervous system activity, with sustained catecholamine elevation, increasing vascular tone.
-Severe endothelial dysfunction: low NO, high endothelin-1.
-Increased hematocrit and blood viscosity, raising flow resistance.
Trenbolone users often report internal heat sensation, resting palpitations, cranial pressure, insomnia, and elevated diastolic pressures.
It’s common to see pressures of 130-150/85-95 mmHg, even in well-managed athletes.
What makes it so aggressive for BP?
-Intense indirect mineralocorticoid effect: although it doesn’t bind to classic mineralocorticoid receptors like aldosterone, it alters sodium-potassium balance and promotes sodium retention.
-Chronic vasoconstriction: trenbolone enhances sympathetic nervous system activity, with sustained catecholamine elevation, increasing vascular tone.
-Severe endothelial dysfunction: low NO, high endothelin-1.
-Increased hematocrit and blood viscosity, raising flow resistance.
Trenbolone users often report internal heat sensation, resting palpitations, cranial pressure, insomnia, and elevated diastolic pressures.
It’s common to see pressures of 130-150/85-95 mmHg, even in well-managed athletes.
3.4 - Nandrolone
Although nandrolone is considered “milder” in androgenic effects, it has a notable hypertensive profile:
Mechanisms:
-Strong water-sodium retention through aldosterone-like effect.
-Long-term reduction of vascular elasticity: nandrolone alters endothelial architecture and promotes vascular fibrosis with chronic use.
-Alters lipid profile: lowers HDL and raises LDL, although less than orals like Dianabol or oxymetholone.
It usually produces a moderate but sustained increase in BP that, if not monitored, becomes chronic over time.
Mechanisms:
-Strong water-sodium retention through aldosterone-like effect.
-Long-term reduction of vascular elasticity: nandrolone alters endothelial architecture and promotes vascular fibrosis with chronic use.
-Alters lipid profile: lowers HDL and raises LDL, although less than orals like Dianabol or oxymetholone.
It usually produces a moderate but sustained increase in BP that, if not monitored, becomes chronic over time.
3.5 - Boldenone
Boldenone is known for raising hematocrit and blood viscosity, which indirectly contributes to elevated blood pressure.
Why?
The increase in red blood cell mass makes the blood thicker, increasing resistance through vessels and raising cardiac workload.
It can also cause mild water retention, though less than the previous compounds.
In long or poorly controlled cycles, it can contribute to hypertension, especially if hematocrit exceeds 55%.
Why?
The increase in red blood cell mass makes the blood thicker, increasing resistance through vessels and raising cardiac workload.
It can also cause mild water retention, though less than the previous compounds.
In long or poorly controlled cycles, it can contribute to hypertension, especially if hematocrit exceeds 55%.
3.6 - Testosterone
Pure testosterone has a moderate impact on BP, but not harmless:
At well-adjusted TRT doses it rarely causes problems, but at supraphysiological doses (500 mg/week or more):
-It increases sodium and water retention.
-It Activates the sympathetic system.
-It Lowers HDL.
Its effects are dose-dependent and become more pronounced when stacked with other compounds.
At well-adjusted TRT doses it rarely causes problems, but at supraphysiological doses (500 mg/week or more):
-It increases sodium and water retention.
-It Activates the sympathetic system.
-It Lowers HDL.
Its effects are dose-dependent and become more pronounced when stacked with other compounds.
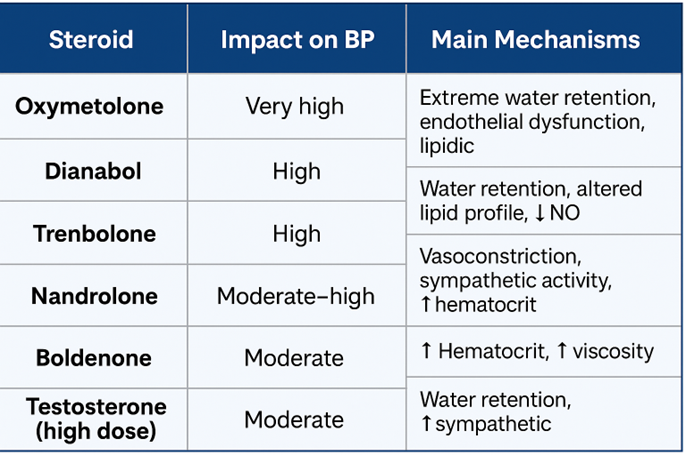
SUMMARY TABLE
4 - How to prevent damage
BP control in an AAS user must be an absolute priority. And that starts with proper monitoring
Measurement should be systematic: 5-10 minutes rest beforehand, three readings per session, avoiding stimulants before measurement, using an approved upper arm BP monitor.
In cases of long cycles or polypharmacy, 24h ambulatory BP monitoring (ABPM) is ideal to detect abnormal patterns.
Non-pharmacological prevention includes:
-Strict dietary sodium control: not just ditching the salt shaker, but reviewing processed foods, sauces, industrial seasonings.
-Increase intake of potassium, magnesium, and calcium, which counter sodium retention.
-Prioritize regular cardio, not just as a body composition tool but as an active cardiovascular health measure.
-Avoid alcohol, moderate caffeine, and avoid NSAIDs unless truly necessary.
When BP rises and crosses the safety line, medications come into play:
-ACE inhibitors and ARBs are preferred for their kidney and heart protective properties.
-Beta-blockers help when the heart rate is high or signs of cardiac overload appear.
-Calcium channel blockers may be necessary in cases of resistant hypertension.
No supplement replaces real treatment. Olive extract, nattokinase, coenzyme Q10 can support, but do not replace medication when the risk is high.
In cases of long cycles or polypharmacy, 24h ambulatory BP monitoring (ABPM) is ideal to detect abnormal patterns.
Non-pharmacological prevention includes:
-Strict dietary sodium control: not just ditching the salt shaker, but reviewing processed foods, sauces, industrial seasonings.
-Increase intake of potassium, magnesium, and calcium, which counter sodium retention.
-Prioritize regular cardio, not just as a body composition tool but as an active cardiovascular health measure.
-Avoid alcohol, moderate caffeine, and avoid NSAIDs unless truly necessary.
When BP rises and crosses the safety line, medications come into play:
-ACE inhibitors and ARBs are preferred for their kidney and heart protective properties.
-Beta-blockers help when the heart rate is high or signs of cardiac overload appear.
-Calcium channel blockers may be necessary in cases of resistant hypertension.
No supplement replaces real treatment. Olive extract, nattokinase, coenzyme Q10 can support, but do not replace medication when the risk is high.
5 - Consequents
Ignoring elevated BP during an AAS cycle is like ignoring a fire starting to spread in the forest. At first it doesn’t seem serious. But damage accumulates.
The heart becomes rigid. The kidney starts filtering worse. The endothelium is damaged. The arteries fill with plaques. And when the event comes — heart attack, stroke, kidney failure — many times it’s too late.
Erectile dysfunction, which many users try to combat with more drugs, is itself an early marker of endothelial damage from hypertension and dyslipidemia associated with AAS use.
6 - Conclusion
Hypertension in the context of steroids is not optional: it is foreseeable, preventable, and must be monitored. If it’s not measured, it’s not controlled. If it’s not controlled, it causes silent but deadly damage
The bodybuilder who wants to last years in the game has to take care of what isn’t visible: their blood pressure, heart, kidneys. Only then will the physique seen on the outside be synonymous with health and not silent disease.
The bodybuilder who wants to last years in the game has to take care of what isn’t visible: their blood pressure, heart, kidneys. Only then will the physique seen on the outside be synonymous with health and not silent disease.